Degeneration of corticobulbar pathways to v,vii,x,xi,xii: Rather than the corticobulbar tracts: Lower motor neurone signs absent:
Lower motor neurone signs present: Jaw jerk (+) jaw jerk (n) spastic dysarthria: Decreased jaw reflex, progressive bulbar paralysis & tongue paralysis symptom checker:
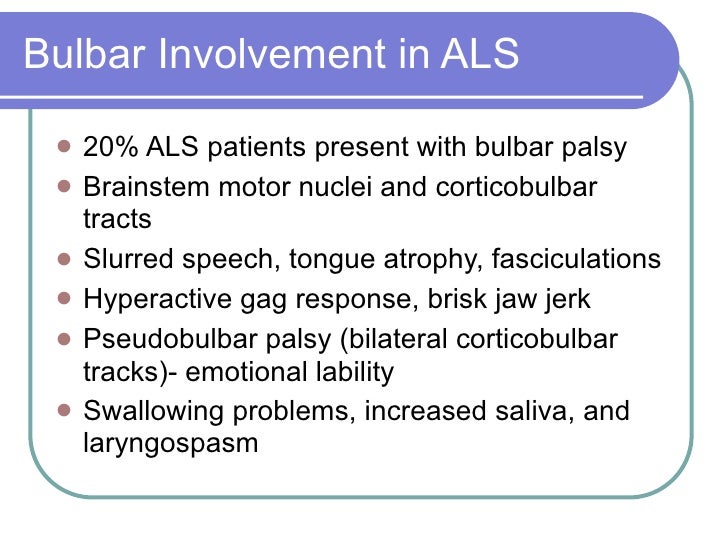
Possible causes include amyotrophic lateral sclerosis. Check the full list of possible causes and conditions now! Talk to our chatbot to narrow down your search.
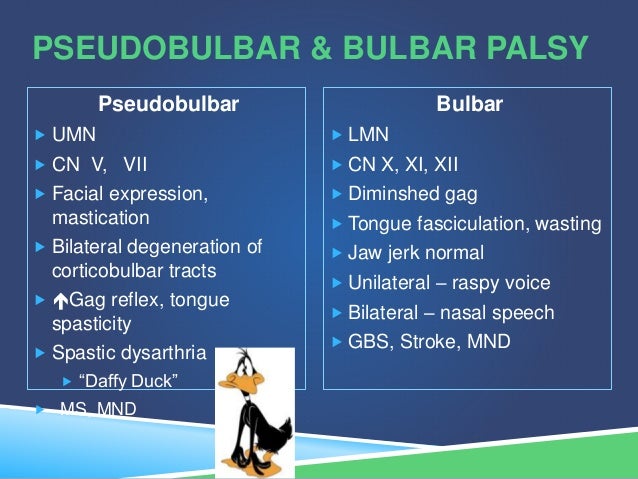
Informed consent has been taken from the patient. Lower motor neuron signs (atrophy and fasciculations of the tongue, absent gag reflex) differentiate bulbar palsy from pseudobulbar palsy, which presents with upper motor neuron signs (spastic tongue, exaggerated gag, and jaw jerk reflexes). Diagnosis is mainly clinical.
Csf analysis and mri of the brain help identify the etiology. There are two principal types of bulbar palsy: Progressive bulbar palsy (pbp) and pseudobulbar palsy.
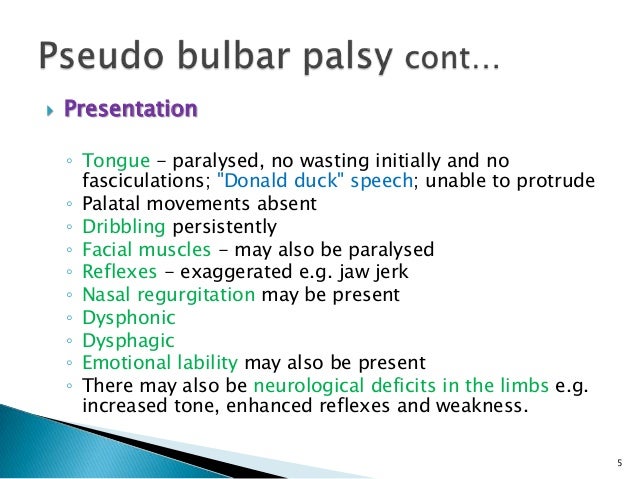
In both, the outstanding symptoms are dysphagia and dysarthria. There is often an exaggerated jaw jerk, a hyperactive gag reflex and frontal release signs such as snout and suck reflexes. Pseudobulbar affect is common. (1)
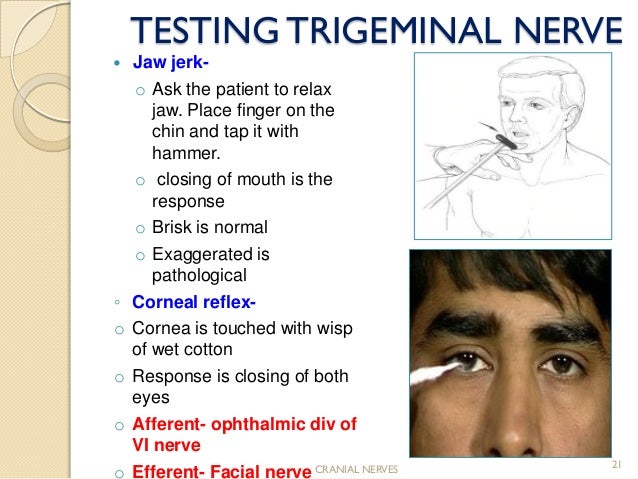
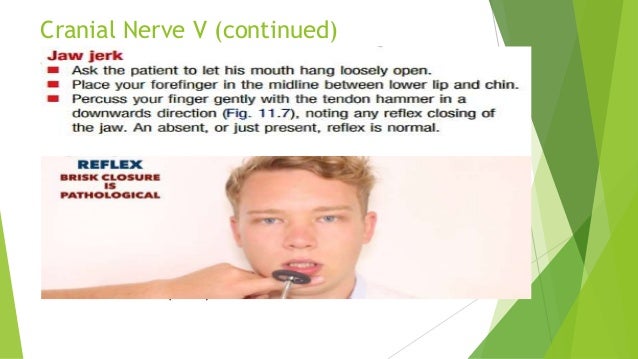
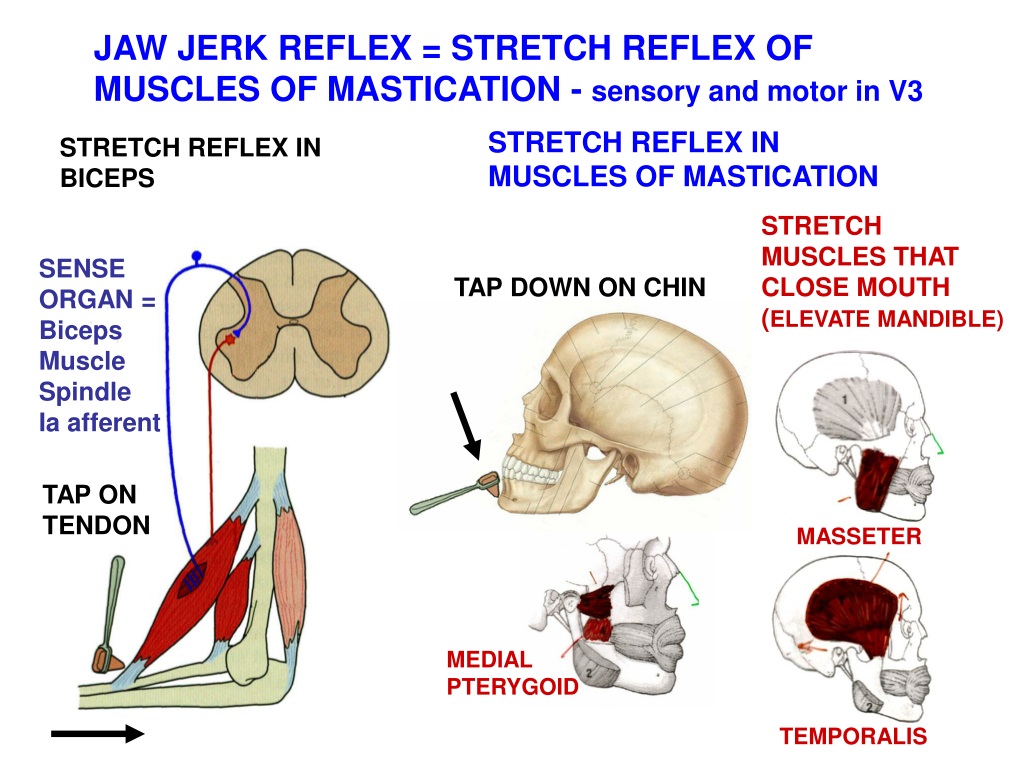
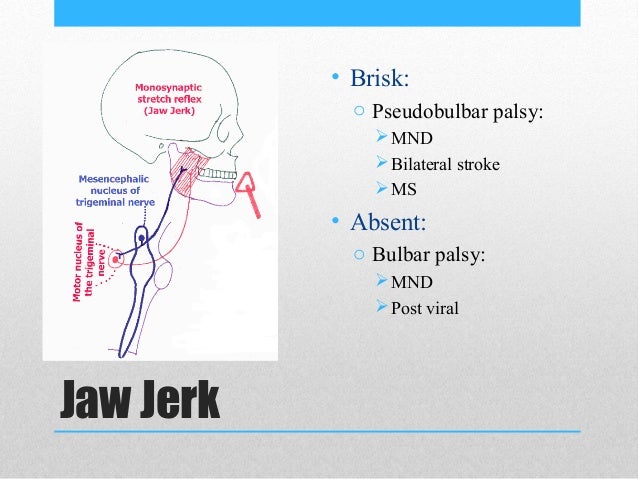
The jaw jerk reflex or the masseter reflex is a stretch reflex used to test the status of a patient's trigeminal nerve (cranial nerve v) and to help distinguish an upper cervical cord compression from lesions that are above the foramen magnum. The mandible—or lower jaw—is tapped at a downward angle just below the lips at the chin while the mouth is held slightly open. In contrast to bulbar palsy, the reflex movements of the soft palate and pharynx are frequently hyperactive.
The jaw jerk is brisk. Frontal signs (grasp, snout, suck, and glabellar reflex) may be present. Emotional incontinence with exaggerated crying (or, less often, laughing) is also common and may be due to disruption of frontal efferents.
Bulbar palsy is the result of diseases affecting the lower cranial nerves, whereas pseudobulbar palsy results from disease of the corticobulbar tracts. Nasal regurgitation may be present. How much can one rely on exaggerated deep tendon reflexes.
Bulbar palsy (lmn) nasal speech which lacks modulation. Speaks in short phrases. Slurred words, especially of the consonants.
Wasted, flaccid, fasciculating tongue. An exaggerated jaw jerk, sometimes appearing with clonus (see below), implies bilateral disease above the level of the pons (e. g. , pseudobulbar palsy). In patients with spastic tetraparesis, for example, an exaggerated jaw jerk excludes cervical cord disease and points to pyramidal tract disease above the pons.
While not part of a standard neurological examination, testing this reflex is done when there are other signs of damage to the trigeminal nerve. A normal jaw jerk reflex points diagnosis toward cervical spondylotic myelopathy, and away from multiple sclerosis or amyotrophic lateral sclerosis. The jaw jerk reflex is enhanced in spastic bulbar palsy.
Other clinical signs associated with bulbar palsy include a nasal speech that lacks in modulation (e. g. Controlling or adjusting of one’s speech), difficulty with all consonants, an atrophic (wasting) tongue, drooling, weakness of the jaw and facial muscles, a normal or absent jaw jerk (upward jerk of the jaw upon striking the chin) and an. A bulbar palsy is a lower motor neuron lesion of cranial nerves ix,.
Brisk jaw jerk reflex symptom checker: Possible causes include autosomal recessive spastic paraplegia type 50. Check the full list of possible causes and conditions now!
[11][12] diagnostics bulbar palsy and [amboss. com] on physical examination, there is a brisk jaw jerk. Other facial reflexes also become exaggerated. There are retained or.
Most common types of bulbar palsy are progressive bulbar palsy (pbp) and pseudobulbar palsy. There is mostly an exaggerated jaw jerk, a hyperactive gag reflex and frontal release signs such as snout and suck reflexes. Pseudobulbar palsy mostly occurs in multiple cerebral infarctions related condition such as encephalitis, ms, trauma.