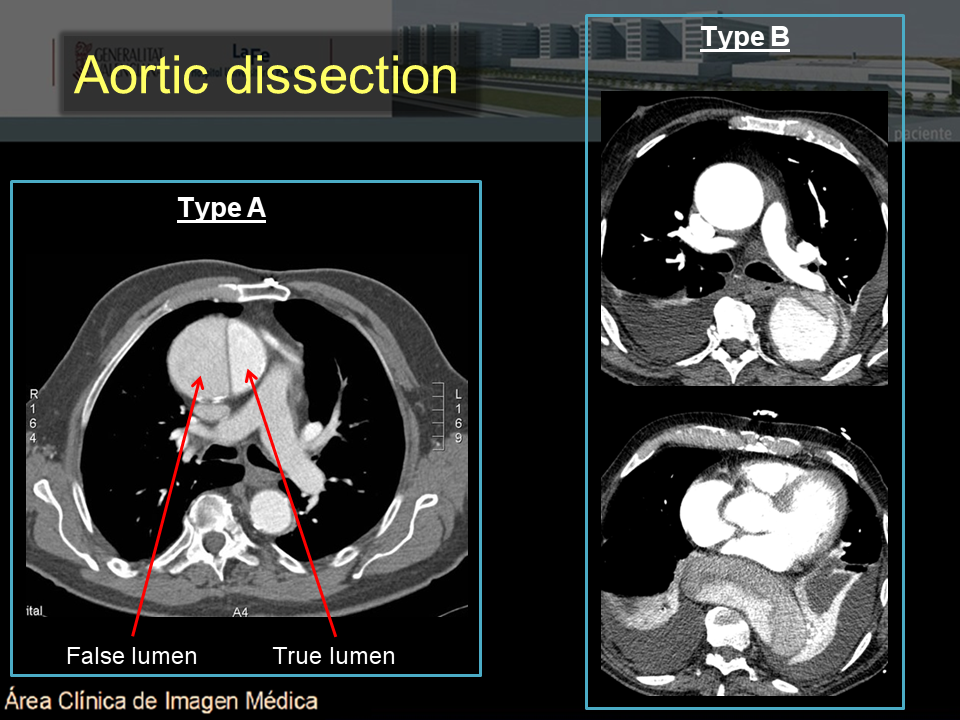
On the left an aortic dissection is seen with a large false lumen. The compressed true lumen is seen on the inner side and is brighter than the false lumen. Thrombus formation within the false lumen.
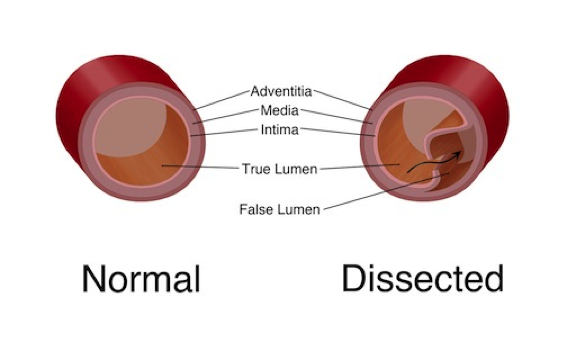
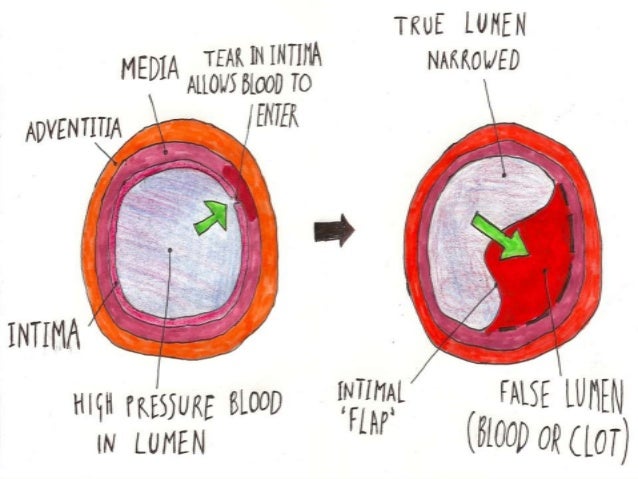
The true lumen usually is smaller as the false lumen wedges around the true lumen due to permanent systolic pressure. The false lumen usually. The goals of open aad repair and endovascular aneurysm repair are to prevent lethal complications, resect the entry tear, and redirect the blood flow to the true lumen.
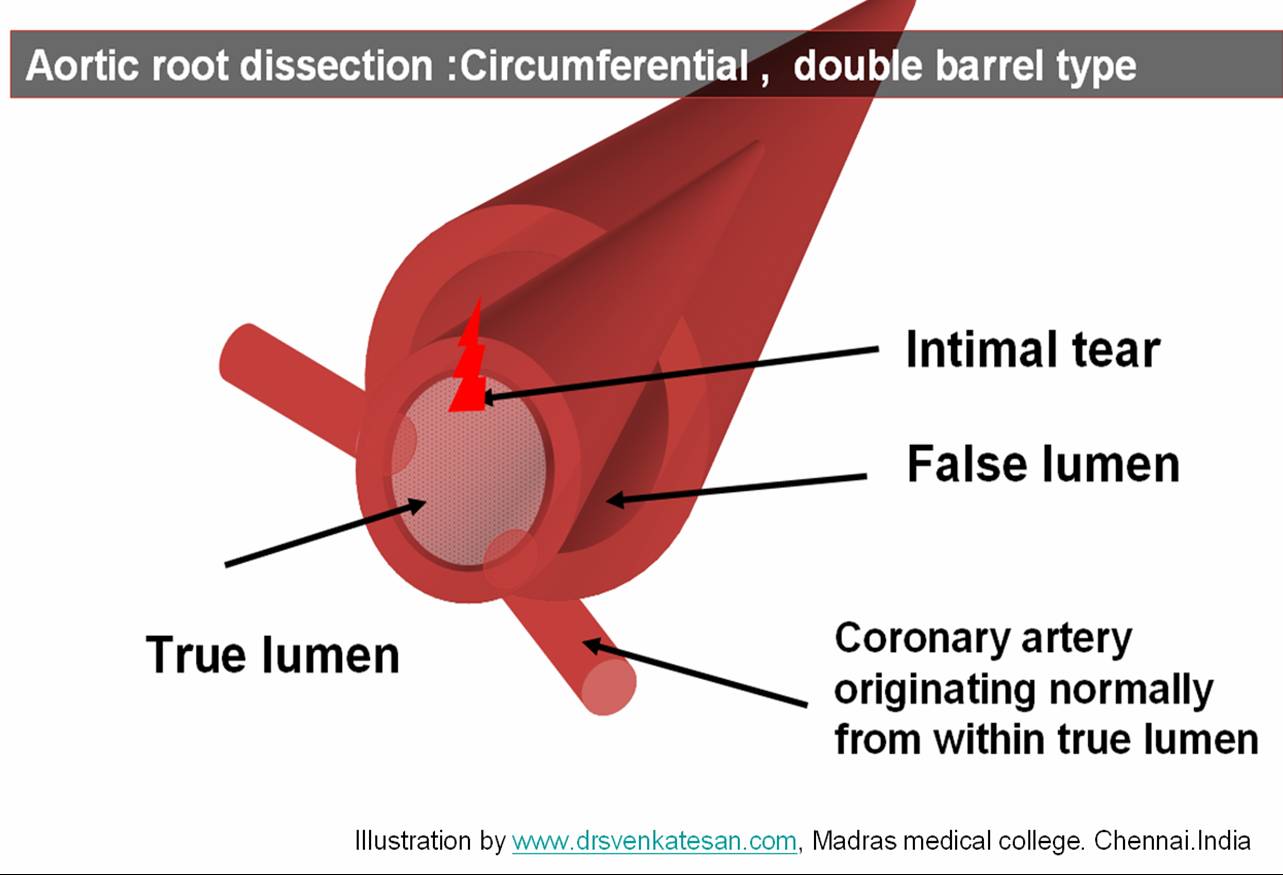
22 blood flow through the false lumen will be altered by resection of the primary tear and aortic reconstruction, because thrombosis of the false lumen is promoted. The classic false lumen is crescent shaped. True lumen is either round or oval (gibbous moon) tunction between false and true lumen has some characteristic feature. it mimics the letter y.
The mainstem of y correspond to main ( normal full thickness)aortic wall of the true lumen. the oblique lines represent the outer wall of the false lumen and. To determine the intravascular ultrasound (us) features of aortic dissection that can be used to differentiate the true from the false lumen. Intravascular us and aortography were performed in 34 patients with aortic dissection.
Aortic necropsy specimens were available in five patients. True and false lumina in. Aortic dissection is associated with a high mortality rate and has been increasingly treated with endovascular therapy.
False lumen (fl) patency has been shown to be associated with worse outcomes. Fl interventions that incorporate the flirt (fl intervention to promote remodeling and thrombosis) concept have been associated with improved aortic. The purpose of this study was to determine which ct findings are reliable indicators of the true or false lumen in an aortic dissection.
B aortic dissection treated medically between 2000 and 2006 were followed with serial mdct angiography and mr angiography scans during the chronic phase (mean, 5. 3 scans per patient; True v/s false lumen of aortic dissection. Two lumens separated by dissection flap:
Less dense contrast due to delayed opacification. The purpose of this study was to determine which ct findings are reliable indicators of the true or false lumen in an aortic dissection. The beak sign and a larger.
The purpose of this study was to determine which ct findings are reliable indicators of the true or false lumen in an aortic dissection. Features generally indicative of the true lumen included outer wall calcification. This considerable change on the aortic morphology alters hemodynamic features dramatically and, in the case of rupture, induces markedly high rates of morbidity and mortality.
In this study, we. The false lumen is usually larger than the true lumen in classic dissection (figures 5. 10 and 5. 11). In the study of lepage et al. 33, at one quarter of the distance along the dissected length of the aorta, the larger lumen was the false lumen in 85% of the acute cases and 83% of.
If one lumen wraps around another in the aortic arch, the inner lumen is the true lumen. Outer wall calcification always indicates the true lumen in an acute dissection. However, the outer wall of the false lumen can calcify in a chronic dissection if the false lumen lining endothelializes.
Features of the false lumen in an aortic. The acute angle or beak (b, arrowhead) marks the junction of the dissection flap with the aortic wall and lies within the false lumen. Cordlike remnants of media, aortic cobwebs, are a reliable marker of the false lumen (a, arrows).
Characteristically, they stretch from the dissection flap covering the true lumen (a, arrowheads. 3 persistent patent false lumen in the descending aorta is common in both types and has been strongly associated with poor prognosis.